Joe Miller is the
Vice President of Business Development for Interactive
Metronome, Inc. Joe’s background in the healthcare
industry includes sales, marketing and product
development. Joe was one of the first healthcare
professionals responsible for introducing VitalStim
where he managed. Communications and Corporate
Relations. Joe developed and managed the national
campaign to introduce The Hand Mentor to the
rehabilitation industry including managing a continuing
education (CE) organization responsible for implementing
neuro-rehab courses to therapists across the United
States. Joe is responsible for business development
activity in the western United States as well as further
developing National Corporate Accounts.
New
course locations added!
Date
Location
3/15
Cleveland, OH
3/15
Spokane,
WA
3/29
San
Francisco, CA
3/29
Kansas
City, KS
4/5
Portland,
ME
4/5
Long
Beach, CA
4/5
Salt Lake
City, UT
4/12
Atlanta,
GA
4/12
Chicago,
IL
4/19
Ft.
Lauderdale, FL
4/19
Spokane,
WA
4/26
Tampa, FL
4/26
St. Paul,
MN
4/26
Houston,
TX
5/3
Charlotte, NC
5/3
Kansas
City, KS
5/10
New
Orleans, LA
5/10
Phoenix,
AZ
5/17
Charleston, SC
5/17
Port
Orchard, WA
5/31
Naples,
FL
5/31
Biloxi,
MS
5/31
San
Antonio, TX
6/7
Orlando,
FL
6/7
San
Diego, CA
6/14
Indianapolis, IN
6/14
Portland,
OR
6/21
Toronto,
Canada
6/21
Lincoln,
NE
6/28
Hartford,
CT
6/28
Birmingham, AL
6/28
Dallas,
TX
The cost 3 weeks
before the course date is
$205
for an individual
and $180 for a group of 3 or more.
Within 3 weeks of the course the regular price
is $225
for an individual
and $200 for a group of 3 or more.
*Don't see a course
in your area?
Click here to e-mail a Private Course
request (Please include 3 course dates you are
interested in.
*Note:
Courses must be scheduled at least 45 days in
advance) or call 877-994-6776 opt 4 (US Only) or
954-385-4660 opt 4
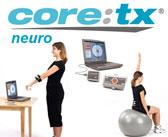
The
Core:Tx ® is versatile with 14 pre-selected
movements and the ability to add any new movements
of functional motor patterns. These exercises can be used to
facilitate neuro-muscular control and carry-over to
functional task performance while at the same time
measuring progress.
Cost: $1895 + $300 Annual
Licensing Fee Includes: Base station,
Transceiver, USB Cable, Three AAA batteries, Six straps & one
strap extension, Software
installation CD, Core:Tx
®
user guide, &
Core:Tx
®
quick start guide.
Call 877-994-6776 to
Order today
Order
Today!
The IM Professional
Conference DVDs are available for purchase.
Cost: $160 (Includes DVD
Set) or $100 for additional CEUs (your facility must
already own the DVD set)
Contact Hours:16.0
AOTA
If you are interested in earning ASHA CEUs please
contact Bricole Plew for details at 877-994-6776 x237
Introduction to IM & Patient Testimonial-
Matthew Wukasch, CEO & Kelly Buggle,
TBI Patient
The
Brain Clock: An Overview of Contemporary
Research & Theory
Regarding the
Neuroscience of Brain-based Interval
Timing & Its Relevance to Learning &
Rehabilitation- Dr. Kevin McGrew
Effect of Interactive Metronome on
Auditory Processing- Dr. Joel Etra,
SLP.D, CCC-SLP
The Use
of IM in Infancy- Lucy Barlow, SLP
Strategies to Preserve Function and
Independence: IM and Parkinson’s
Disease- Karen Farron, OT
Integrating IM in our
Treatment of Autism, Apraxia,
ADHD, CAPD, and Reading
Disorders: Digging Deeper-
Janey Tolliver, SLP
Functional Mobility with
Neurologically Impaired
Adults– Shelley Thomas,
PT
A Pilot Study- The Use
of IM in Public Schools–
Deb Law, OT, Patricia
Snowden, SLP, & Amy
Mason, SLP
Individualizing IM
Treatment for Older Adults- Dr. Leonard Trujillo
Advanced IM Best
Practices for the
Aphasic/Apraxic
Population– Dara
Coburn, SLP
Use of IM to
Improve Switch
Activation and
Ambulation in a
Young Near
Drowning Victim-
LorRaine Jones
SLP
Making It Work: Module 1-
Improving Visual Attention &
Processing with Visual-Only
IM- Amy Vega, SLP
Making It Work: Module
2-
Improving Visual
Attention, Processing, &
Executive Functions With
IM - Supplementary
Tasks- Amy Vega, SLP
Making It Work: Module 3-
Advanced IM
Practices for Correcting Dissociative Responses &
Improving Upper Extremity Coordination- Linda Rubin,
OT
Making It Work:
Module 4- Advanced IM
Practices for
Lower Extremity
Coordination &
Balance- Linda
Rubin, OT
Panel Discussion
featuring all
Presenters and
Final Thoughts on IM
Quick
Reference Sheet for Download
Having problems remembering when a
patient should be moved to the next phase of treatment or need a
little help deciding what to do when a patient is having a
performance problem?
That's what we're here for. Our Clinical Education department has
developed a quick reference sheet to help you.
If you
are an Interactive Metronome Provider and have
recently upgraded your
computer to the Vista Platform, please contact our
Support Department to have a new disk mailed to you.
Please note that you must have the latest version of IM
(8.0) to get this upgrade.
If you didn't get a chance
to attend this year's American Physical Therapy
Association's (APTA) Combined Sections Meeting, held
February 6-9 in Nashville, Tenn., then here's your
chance to see an exclusive interview with Matthew
Wukasch, CEO of Interactive Metronome, at the APTA CSM
2008 annual conference.
An excerpt from the book "Sensory Integration Theory and
Practice"
By Anita C Bundy, Shelly J. Lane and Elizabeth A Murray
Although very different from
sensory integrative-based approach, we have recently
found that the Interactive Metronome, a computer-based
training program, is helpful for improving bilateral
coordination. The Interactive Metronome involves
matching bilateral movements to auditory cues given
through headphones (Shaffer et al., 2001). This training
is also helpful for improving timing, rhythm, and
planning and sequencing of movements and, therefore
addresses many axis of praxis (Koomar et al., 2001). The
Interactive Metronome may be most beneficial after a
client has participated in sensory integrative-based
intervention.
E
Effect of IM on normal aging population
Q: How does IM effect the normally aging
population?
A: Dr. Leonard Trujillo completed a study on
typically aging adults ages 55-68 which examined the
transfer effect of IM to fine motor skills. He found
that 9 sessions of IM (focusing only on hand tasks)
resulted in statistically significant gains in fine
motor skills as measured by the 9-Hole Peg Test. Gains
were demonstrated bilaterally. Dr. Trujillo has proposed
future research. His area of interest is in the at-risk
older driver. His paper is being submitted for
publication. IM is used in conjunction with drivers
evaluation and training programs as it improves the
motor and cognitive abilities necessary for safe
driving. Contact
Amy Vega, IM Clinical Education Director, for an
interesting paper on cognitive decline with aging by
researchers at U of M. Brain structures implicated in
mental decline with aging are the same structures
impacted by IM (dorsolateral prefrontal cortex,
cerebellum, etc).
F
FastForward
Q: Which is more effective for reading,
FastForward or IM?
A: It is more effective to first improve timing
and phonological awareness via IM, then proceed with
intensive reading instruction, like FastForward.
Frequency
Q: What is the optimal frequency? Can gains be
seen if patient only receives 1-2 sessions per week?
A: Frequency and intensity of therapy dictates
pace of therapy and how quickly outcomes are realized.
The more frequent and the more
intense (i.e., more repetitions each session), the
faster and more complete the outcomes. Obviously, if
less is provided, then outcomes will take longer to
realize and if frequency is too low, full outcomes may
not be realized. Each individual’s needs vary, so
determine the frequency and intensity based upon the
individual. One time per week, while certainly helpful
and better than nothing, may not be enough for many
patients.
In adult outpatient rehab settings that accept Medicare,
the maximum frequency allowed is 3x/week. Inpatient
rehab is 5-7x/week. Pediatric rehab may be 3-5x/week in
outpatient, 5-7x/week in inpatient.
Duration of sessions vary depending upon setting
(inpatient versus outpatient, age, and individual
patient characteristics) Short sessions of 15-30 min
3x/week have been reported to be effective for some
patients.
Funk Period During Reorganization
Q: Do patients go through a period of regression
during IM as neurological reorganization is taking
place?
A: This frequently happens. Regression can occur
in speech fluency, language, fine/gross motor,
social/emotional, and behavioral skills. This is
temporary and IM should continue. Also: Always monitor
the frequency and intensity of treatment to make sure it
is not too much for the patient.
G
Gait Switch
Q: What is the IM Gait Switch?
A: Plastic shoe insert with wireless IM trigger
in the heel. One goes in each shoe. As the patient
walks, he receives feedback regarding symmetry, timing,
and rhythm of gait.
Grant Writing
Q: Does IM provide assistance or a template for
grant-writing?
Q: How does IM work if you are providing all
hands-on assist?
A: As the provider, you provide hands-on feedback
for timing to your patients as needed. Some patients,
particularly young ones, will need complete hands-on
assist. It is important for your timing to be in the
20’s or lower if at all possible before you provide
hands-on assist to patients. Not sure exactly how it
works, anecdotal reports indicate that pediatric
patients who receive total hands-on assist make
substantial gains in sensory, motor, cognitive, and
language skills.
Headphones
Q: Can you use other types of headphones with IM?
A: Yes you can use headphones such as ipod ear
buds, open systems, audiology headphones that fit
snugly, etc.
Hearing Impaired
Q: How do you adjust the volume for hearing
impaired patients?
A: If no hearing aids, use headphones & raise
Master Volume a notch at a time & check to see if
patient can hear the individual sounds. Note: When
clicking on each sound tab, that sound will play in only
one of the ears. To check the other ear, turn the
headphones around so other ear can hear the sounds.
Raise Master Volume to as high as 11 if needed. Do not
go much higher than that as it gets very loud and may
damage hearing.
If hearing aids are worn, use speakers instead of
headphones and raise Master Volume as high as
needed. Place speakers so they are at head level and
patient is facing them in order to localize if sound is
coming from the left or right side. Placement of
speakers on a medical bedside table that can be raised
or lowered is optimal so that speakers are at head/chest
level when patient is seated or standing. Tip: Velcro
speakers to the table to prevent them from falling off.
I
IM Settings
Q: How do you know when you need to modify IM
settings?
A: Observe the patient. Here are some examples:
You will see that the tempo is either too fast for the
patient and he can’t keep up. Or you will see that the
patient is too fast and cannot slow down to get into
sync with 54 beats per minute. In one case, you will
reduce the tempo and in the other you may opt to
increase the tempo to facilitate success with the
program initially.
Before turning on the guide sounds, you may notice that
that patient is scoring 256ms. You may reason that if
you have the Difficulty set at 100, the patient will
hear the buzzer constantly and get frustrated. So you
will adjust the difficulty to an easier setting, like
300.
Once the guide sounds are learned, you may notice the
patient stays within a certain ms range now, but seems
to plateau. He can only get his score to 55ms. You now
have the Difficulty back to 100. The patient may need
you to nudge him in the direction of Super-Right-On, so
you adjust the Difficulty to 80.
Insurance
Q: Is IM reimbursed by insurance?
A: IM is typically reimbursed by insurance if it
is provided by an allied health professional, physician,
chiropractor or psychologist/neuropsychologist who is on
the insurance companies panel of providers (for this,
you must apply to each individual insurance panel), and
it is billed using the appropriate CPT code (i.e., for
OT: therapeutic activities, therapeutic exercises,
neuromuscular reeducation, cognitive development, etc).
IM does not have it's own CPT code, so you should never
ask for authorization for "IM Treatment" or "Interactive
Metronome Therapy" from the insurance company. To be
reimbursed by insurance, you will need a prescription
from a physician for "OT/ST/PT eval and treat," that
includes the treatment frequency and duration, and that
the treatment is medically necessary.
To maximize reimbursement, you must also be sure the
appropriate diagnosis code is used, perform appropriate
pre and post objective and functional assessments,
document sound rationale for the treatment (how it will
improve the patient's function), document functional and
measurable goals, and functional outcomes of
treatment. You are better off using terminology that
describes OT/ST/PT eval and treat, rather than IM. IM
will simply be part of your treatment approach and may
be combined with other approaches to achieve therapeutic
outcomes. This will help prevent insurance companies
from labeling your treatment as experimental.
Your documentation
(initial evaluation, progress reports, and discharge
summary) will also facilitate reimbursement as long as
it includes the following information:
Patient demographics
(Name, DOB, Age)
Dates of service
Medical reason for
needing OT (insurance will only pay for treatment
that is medically necessary)
Medical diagnosis
and code
Treatment diagnosis
and code
Medical history
(date of onset, previous therapies, medical
complications, etc)If patient has had OT before and
his returning to OT to receive IM, then state that a
therapeutic approach shown to improve ________ was
not available to the patient previously, so patient
is returning to receive this therapy in order to
improve ______.
Objective
assessments administered, results, and
interpretation
Functional
(clinical) observations and assessments
Measurable and
functional short & long-term goals
Estimated treatment
frequency and duration (that is reasonable and in
line with customary OT services)
Therapists name,
credentials, license #, and signature
If you are not on an
insurance panel, patients who submit your report and
required paperwork to their insurance company for
reimbursement, must usually get pre-approval for therapy
from the insurance company for an "out-of-network
provider." Many insurance companies require their
insured to stay within their provider network. Often, if
there is a provider within the insurance network that
can provide the same therapy for the patient, the
insurance company will deny out-of-network benefits and
refer them to a therapist in network. You may need to
make the case, then, that you are providing a service
that the in-network therapists cannot provide, namely
Interactive Metronome.
For this, you will need to draft a letter to the
insurance company (probably with more meat than you are
currently doing) to convince the insurance company to
pay for your services.
Contact Amy Vega, IM Clinical Education Director for
research that you can cite (there is MUCH more research
& information supporting he efficacy of IM than
previously).
Many insurance companies do not cover disorders that are
considered “developmental,” regardless of the
intervention. This may include learning disabilities,
dyslexia, Sensory Processing Disorder, ADHD, Autism,
etc.
Integrating IM into
Practice
Q: How do you integrate IM into a treatment plan?
A: IM is only part
of a more comprehensive treatment plan. Depending upon
the patient, IM may be the only treatment received
initially followed by reassessment and other therapies
as needed. i.e., TBI patient does IM to improve
attention, processing, executive functioning, working
memory, behavioral self-regulation, and reading.
Reassessment reveals continued memory deficit. Therapy
transitions to training of compensation device for
memory such as blackberry.
Other patients may begin their therapy session with
short IM tasks to improve alertness/arousal, then
therapy proceeds with other tasks. i.e., man with stroke
in inpatient rehab setting who is lethargic and has
difficulty with active participation in therapy. IM is
done for 10-15 min followed by dysphagia therapy
A child with sensory processing disorder may begin the
treatment session with vestibular and proprioceptive
activities, followed by brushing, then IM for 15 min
with sensory moderators as needed for sensory
defensiveness. The IM machine will be brought to the
sensory gym if not too distracting for the child, rather
than taking the child away to a quite, sterile room.
Look for
more FAQs of the
alphabet in the April eNews
13794 NW 4th
Street
• Suite 204 • Sunrise, FL • 33325 • www.interactivemetronome.com • 877-994-6776 • 954-385-4660